Notes on Proximal Convoluted Tubule (PCT) – Reabsorption & Secretion MCQ with answer and Lecture for NEET, GPAT
Notes on Proximal Convoluted Tubule (PCT) – Reabsorption & Secretion
Overview of the PCT
- Location: First segment of the nephron tubule, following Bowman’s capsule.
- Structure: Composed of simple cuboidal epithelium with extensive microvilli (brush border) to maximize surface area for reabsorption and secretion.
- Function: Primary site for reabsorption of filtered substances and secretion of waste products into the tubular fluid.
Get full Lecture Series of Urinary System: Click Here
Reabsorption in the PCT
- Definition: Process of moving substances from the tubular fluid back into the peritubular capillaries (blood).
- Key Characteristics:
- Reabsorbs ~65-70% of the glomerular filtrate.
- Bulk reabsorption occurs here, driven by active and passive transport mechanisms.
- Substances Reabsorbed:
- Water: ~65% reabsorbed via osmosis, following solute reabsorption.
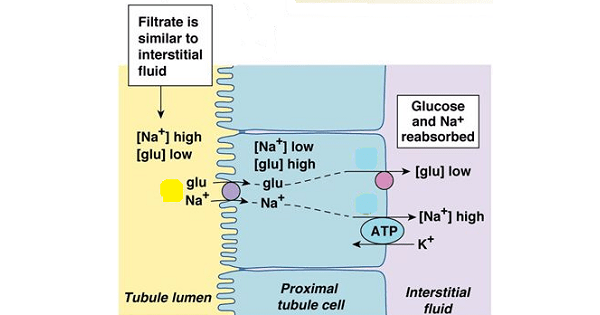
- Glucose: 100% reabsorbed (normally) via Na+/glucose cotransporters (SGLT) in the apical membrane; secondary active transport.
- Amino Acids: 100% reabsorbed via Na+-dependent cotransporters.
- Sodium (Na+): ~65-70% reabsorbed via Na+/K+ ATPase (basolateral membrane) and cotransporters/channels (apical).
- Bicarbonate (HCO3-): ~80-90% reabsorbed; linked to H+ secretion and carbonic anhydrase activity.
- Chloride (Cl-): Reabsorbed passively (paracellular) or via Cl-/HCO3- exchangers.
- Potassium (K+): ~65% reabsorbed, mostly passive following Na+.
- Urea: ~50% reabsorbed passively due to concentration gradient.
- Mechanisms:
- Active Transport: Na+/K+ ATPase on basolateral membrane creates a Na+ gradient, driving cotransport of glucose, amino acids, etc.
- Passive Transport: Water, Cl-, and urea follow osmotic/electrochemical gradients.
- Transcellular Pathway: Through cells (e.g., Na+, glucose).
- Paracellular Pathway: Between cells (e.g., Cl-, water).

Secretion in the PCT
- Definition: Process of moving substances from the peritubular capillaries (blood) into the tubular fluid.
- Purpose: Eliminates waste, regulates blood pH, and clears drugs/toxins.
- Substances Secreted:
- Hydrogen Ions (H+): Secreted via Na+/H+ exchanger (NHE) to regulate pH and reclaim HCO3-.
- Ammonium (NH4+): Secreted as part of acid-base balance.
- Organic Acids/Bases: e.g., penicillin, PAH (para-aminohippurate), creatinine; via organic anion/cation transporters (OAT/OCT).
- Drugs/Toxins: Cleared via specific transporters.
- Mechanisms:
- Active transport (e.g., H+ secretion via NHE3).
- Carrier-mediated transport for organic compounds.
Regulation
- Starling Forces: Reabsorption enhanced by high oncotic pressure in peritubular capillaries (due to filtration in glomerulus).
- Hormones:
- Angiotensin II: Stimulates Na+/H+ exchange → ↑ Na+ and HCO3- reabsorption.
- PTH (Parathyroid Hormone): Inhibits phosphate reabsorption.
- Transport Maximum (Tm): Limits reabsorption of glucose/amino acids (e.g., glucosuria in diabetes when Tm exceeded).
Clinical Relevance
- Diabetic Nephropathy: Glucose spills into urine if blood levels exceed Tm (~180 mg/dL).
- Metabolic Acidosis: Impaired HCO3- reabsorption or H+ secretion.
- Drug Clearance: PCT secretion is key for eliminating medications.
Chart: Reabsorption & Secretion in the PCT
| Process | Substance | Amount Reabsorbed/Secreted | Mechanism | Regulation/Notes |
|---|---|---|---|---|
| Reabsorption | Water | ~65% | Osmosis (follows Na+) | Driven by solute gradients |
| Reabsorption | Glucose | 100% (normal conditions) | Na+/glucose cotransport (SGLT) | Tm-limited; spills in diabetes |
| Reabsorption | Sodium (Na+) | ~65-70% | Na+/K+ ATPase, cotransporters | Angiotensin II stimulates |
| Reabsorption | Bicarbonate (HCO3-) | ~80-90% | Na+/H+ exchanger, carbonic anhydrase | Key for pH regulation |
| Reabsorption | Chloride (Cl-) | ~65% | Passive (paracellular), exchangers | Follows Na+ reabsorption |
| Secretion | Hydrogen (H+) | Variable | Na+/H+ exchanger (NHE3) | Regulates blood pH |
| Secretion | Organic Acids (PAH) | Variable | Organic anion transporters (OAT) | Used to measure renal plasma flow |
| Secretion | Drugs (e.g., penicillin) | Variable | Specific transporters | Key for drug clearance |
Multiple-Choice Questions (MCQs)
- What percentage of the glomerular filtrate is typically reabsorbed in the PCT?
- A) 25-30%
- B) 65-70%
- C) 90-95%
- D) 100%
- Answer: B) 65-70%
- Which transporter is primarily responsible for glucose reabsorption in the PCT?
- A) Na+/K+ ATPase
- B) Na+/glucose cotransporter (SGLT)
- C) Na+/H+ exchanger (NHE3)
- D) Organic anion transporter (OAT)
- Answer: B) Na+/glucose cotransporter (SGLT)
- A patient with uncontrolled diabetes mellitus is likely to exhibit:
- A) Increased glucose reabsorption in the PCT
- B) Glucose in the urine due to exceeding Tm
- C) Decreased Na+ reabsorption in the PCT
- D) Increased H+ secretion in the PCT
- Answer: B) Glucose in the urine due to exceeding Tm
- The secretion of hydrogen ions (H+) in the PCT is primarily linked to:
- A) Reabsorption of glucose
- B) Reabsorption of bicarbonate (HCO3-)
- C) Secretion of organic acids
- D) Reabsorption of chloride
- Answer: B) Reabsorption of bicarbonate (HCO3-)
- Which hormone enhances Na+ reabsorption in the PCT?
- A) Parathyroid hormone (PTH)
- B) Atrial natriuretic peptide (ANP)
- C) Angiotensin II
- D) Aldosterone
- Answer: C) Angiotensin II